

What Is The Pagan Significance Of Tearing Out An Animal's Chest Cavity
![]() Open admission peer-reviewed chapter
Open admission peer-reviewed chapter
Review on Ascites in Pets
Submitted: July 26th, 2018 Reviewed: January 28th, 2019 Published: May 14th, 2019
DOI: 10.5772/intechopen.84767

IntechOpen Downloads
i,191
Full Chapter Downloads on intechopen.com
Abstruse
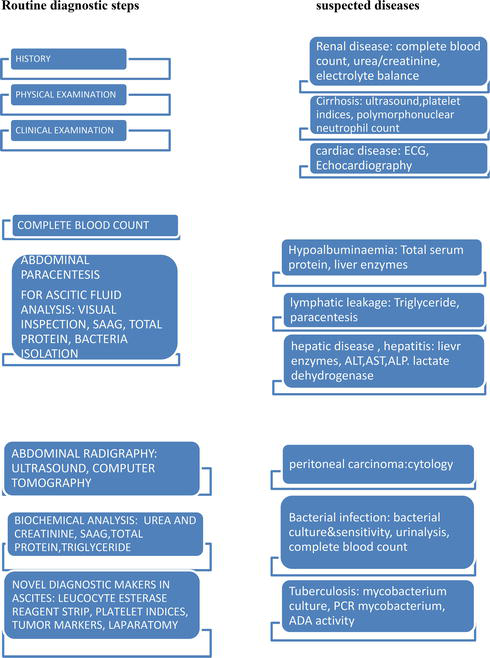
Ascites is ane of the major complications seen in various illness atmospheric condition in pets. Ascites is characterised by distension of the abdomen with accumulation of fluid of various colours and consistencies depending on the cause. The most common causes of ascites in pets include but non limited to the following wellness conditions: hypoproteinaemia, left-sided middle failure, congestive heart failure, cirrhosis, hepatic diseases, renal diseases, ancylostomosis and bacterial infection such as tuberculosis. Pathogenesis of ascites frequently emanate from portal hypertension, cirrhosis, hepatorenal syndrome, etc. Oftentimes the diagnosis of ascites could be cumbersome considering the myriad of diseases implicated in the condition. Standard diagnostic procedures include the post-obit: physical test, clinical examination, ultrasonography, computed tomography, serum ascites albumin gradient (SAAG), biochemical analysis such as triglyceride, urea and creatinine concentration, total poly peptide, etc. Novel diagnostic procedures with possible clinical relevance include the following: leucocyte esterase reagent strip, platelet indices, tumour markers, etc. Diagnosis is made through standard diagnostic procedure, while special cases of idiopathic origin are detected through diagnostic laparotomy. Novel diagnostic procedures such as platelet indices, leucocyte esterase reagent strip and tumour markers would help in easy diagnosis of ascites. Handling of ascites is dependent on identification of the cause of ascites.
Keywords
- ascites
- SAAG
- hepatorenal syndrome
- diuretics
- portal hypertension
- abdominocentesis
- hepatic
- cardiac
- abdominal effusion
- abdominal drops
*Accost all correspondence to: rosemarynwoha@yahoo.com
1. Introduction
Ascites is a term used to depict the condition of accumulation of fluid in the peritoneal crenel. The discussion "ascites" could exist used interchangeably with other terms such as intestinal dropsy, abdominal effusion, peritoneal fluid excess, hydroperitoneum and peritoneal cavity fluid. Ascites represents a grade of general systemic country which could manifest in diverse disease weather in animals. This implies that ascites is merely a clinical manifestation of an underlying disease condition and not a disease in real sense. It further shows that ascites is not a treatable condition except the cause is properly diagnosed and treated appropriately. Ascites is oft diagnosed in dogs between the ages of 5 and 7 years [i]. Cases betwixt the ages of ane and 4 years have as well been recorded. The occurrence of ascites in dogs may be breed dependent with higher incidences in Pomeranian (33.35%) than in Labrador retriever (20%), Boxer (16.66%), Doberman pinscher (13.37%), mongrels (10%) and least in Alsatian (6.66%) [i]. Ascites manifests in several disease atmospheric condition such as hepatic illness, various types of tumour, portal hypertension, alteration in serum protein level (hypoproteinaemia), right-sided center failure, decreased plasma oncotic pressure and increased permeability of capillary endothelium sequel to inflammatory weather, bacterial infection (tuberculosis), kidney malfunction, pre-hepatic portal hypertension, postal service-hepatic portal hypertension, trauma (rupture of lymphatic vessels, blood vessels, urinary bladder),
ancylostomosis peritonitis, bleeding disorders and malnutrition [2, 3]. Other conditions may include heartworm infection and pulmonary stenosis [four]. In full general, cardiac and hepatic disease conditions ranked highest as the cause of ascites in pets. Other manifesting signs which usually signify an underlying disease condition in ascetic pets may include syncope, vomiting, obtundation, seizure, anaemia which manifests every bit pale mucous membrane, weakness and rapid panting. The identification and diagnosis of the cause of ascites may not exist a straightforward procedure and could be complicated due to the several causative factors. The veterinary however has to be guided past the medical aphorism "if y'all hear the audio of hoof first look for a equus caballus before a zebra". This simply means that diagnosis should first with the basis of thorough concrete examination of the entire body and clinical examinations. A well and sequential conduction of physical and clinical examinations serves as a pointer to the underlying cause of ascites. Even so this may not always be so as diagnosis frequently is cumbersome. In such situations diagnosis would include a complete claret count which may reveal evidence of bacterial infection. Intestinal ultrasound/sonography is done to decide the abdominal content and aid in differentiating excess fluid accumulation from abdominal masses and organ enlargement. Knowledge of the blood biochemistry including full protein, albumin, creatinine and urea, liver enzymes and coagulation profile would help in revealing cases of hypoalbuminaemia, hypoproteinaemia and hepatic and kidney diseases [v]. Cardiac diseases may exist diagnosed with the assistance of electrocardiograph. Cardiac auscultation detects cases of cardiac murmurs and arrhythmia. Abdominal paracentesis is a useful process normally carried out to reduce the fluid level and convalesce complications of dyspnea. Paracentesis is a useful procedure in the direction of ascites which is instituted in conjunction with appropriate treatment of the underlying cause. Once advisable diagnosis is made, treatment unremarkably comes easy by alleviating life-threatening conditions such as dyspnea and administering appropriate therapy as the case may exist.
Advertisement
2. Classification of ascites
The purpose of this review is primarily focused on the various causes of ascites with emphasis on the hepatic origin. Based on this premise, ascites is classified broadly into hepatic, pre-hepatic and post-hepatic origin:
-
Pre-hepatic causes emanate from portal vein thrombosis, bacterial infection such equally tuberculosis, malnutrition, hypoalbuminaemia and parasitic diseases such as strongyloidosis and entamoeba [6]. Other causes include trauma or rupture of the lymphatic vessels, blood vessels and urinary bladder, renal failure, lymphoma and neoplasm of diverse kinds including breast, bronchus, ovary, gastric, pancreatic or colonic neoplasms [7]. Up to xx% of neoplastic ascites arise from neoplasm of unknown origin [vii].
-
Post-hepatic causes might include congestive heart failure oftentimes linked with pulmonary hypertension, left-sided heart failure, right-sided heart failure, constrictive pericarditis, Budd-Chiari syndrome and stricture spider web germination in the junior vena cava [viii, 9].
-
Hepatic origin emanates from various hepatic diseases including cirrhosis, portal hypertension and hepatitis. Approximately 85% of portal hypertension results in cirrhosis [8, 9, x].
Earlier classification of ascites was centred on two broad categories, transudates and exudates, based on the total protein concentration of ascetic fluid. High full poly peptide (>2.5 grand/l) was described as exudates, while low total poly peptide (<2.5 1000/l) every bit transudate [11]. Both transudates and exudates were subcategorised into modified transudates and exudates based on the level of total protein concentration in the ascetic fluid. Transudates with <2.five g/l of total protein unremarkably occur with portal hypotension or hypoalbuminaemia [half dozen]. Exudates with >2.v grand/50 of full protein are associated with inflammatory disease conditions such as bacteria tuberculosis, neoplasm of unknown origin, pancreatitis, myxoedema, etc. Notwithstanding, it has been observed that a full protein concentration of <two.5 g/l has an accuracy of only 56% [half dozen] in detecting exudates from diverse weather such as cardiac ascites and patients on diuretics and neoplasms [eleven]. The obvious challenge in the use of total protein concentration paved way to the discovery of serum ascites albumin slope (SAAG) concentration as a more reliable tool in classification of ascites with efficacy ranging from 80 to 100% [11]. With the advent of SAAG, exudate ascites is replaced with (>1.1 g/l) loftier serum ascites albumin slope and transudate with low (<one.one g/l) serum ascites albumin gradient. The SAAG (>1.1 g/fifty) shows higher 94% sensitivity and 90% specificity in detecting portal hypertension than ascetic fluid total protein concentration of <2.5 1000/dl at percent sensitivity and specificity of 78 and 50%, respectively [12]. The prognostic index value of SAAG was at 82–97% compared to full protein concentration at 38–85% [12]. Ascites from cardiac origin produces greater(>2.5g/dl) SAAG compared to cases of cirrhosis [13].
A more recent classification of ascites has endorsed the apply of serum ascites albumin gradient (SAAG) in diagnosis of ascites [14]. The SAAG is derived past subtracting the ascetic fluid albumin level from the serum albumin level obtained on the aforementioned day [14]. Gradients greater than one.1 one thousand/dl indicate ascites of portal hypertension with an accuracy of 97–100% [14]. Gradients less than 1.i g/dl are considered ascites of other sources other than portal hypertension such as neoplasm [15, 16] (Table 1).
| High gradient (>ane.1 one thousand/l) SAAG | Depression slope (<i.1 g/l) SAAG |
|---|---|
| Portal hypertension | Bacterial infection |
| Cardiac diseases | Peritoneal tuberculosis |
| Liver cirrhosis | Pancreatic ascites |
| Myxoedema | Parasitic illness |
| Budd-Chiari syndrome | Ancylostomosis |
| Hepatitis | Nephrotic syndrome |
| Portal vein thrombosis | Trauma and rupture of lymphatic and blood vessels |
| Hypoalbuminaemia | Rupture of the urinary float, left-sided heart failure, correct-sided heart failure, congestive eye failure |
Table 1.
Nomenclature of ascites based on SAAG.
Advertizing
three. Pathophysiology of ascites in cirrhosis
Ascites is ane of the cardinal complications in liver cirrhosis in most patients [8]. Onset of ascites naturally connotes decompensated underlying liver cirrhosis which also signifies poor prognosis with short life expectancy [ten, 17, 18]. Several factors contribute to the evolution of cirrhosis. The eye, for instance, plays an important role through a complex mechanism in the development of liver disease. The mechanism through which the heart and liver affect each other in the evolution of ascites is yet to be fully elucidated [14]. Several circulatory abnormalities observed in cirrhotic patients promulgated the peripheral arterial vasodilation hypothesis proposed in the last century [19]. The circulatory abnormalities manifest as increased cardiac output, portal hypertension, peripheral vascular resistance, arterial hypotension and splanchnic vasodilation [six, 20]. Circulatory abnormalities from cardiac disease affect circulatory volume with a resultant decrease in tissue perfusion affecting majorly the kidney functionality [21]. Earlier in the affliction, renal dysfunction is less expressed; however, with affliction advocacy the patient may feel difficulty in sodium excretion and consequent sodium and water retention [22]. Cirrhotic ascites basically develop from failure in renal excretion of sodium [22]. Different mechanisms also play a role in ascites in cirrhosis. Intrinsic factors including arterial vasodilation bear upon the blood pressure hormones such as the renin-angiotensin-aldosterone arrangement (RAAS) which stimulates sodium reabsorption from the distal nephron [22]. The sympathetic nervous arrangement (SNS) induces renal constriction and sodium reabsorption from the tubules with ascites [23, 24]. The heart, SNS and RAAS play a synergistic function in sodium retentivity and development of ascites in cirrhosis.
3.1 Pathogenesis of portal hypertension in ascites
The portal vein is a major vein comprising of a group of veins which supply the visceral organs including the abdomen, pancreas, intestine, etc. These veins bisect into smaller vessels in the hepatic tissue. Intrinsic factors and disease conditions such equally cirrhosis event in blockage of these tiny veins in the hepatic tissue increasing the blood pressure in the veins with resultant portal hypertension. Other causes of portal hypotension include portal vein thrombosis, schistosomosis, idiopathy, etc. Ascites develops in portal hypertension when the post-sinusoidal gradient is above 12 mmHg [25]. Portal hypertension elevates the hydrostatic pressure within the hepatic sinusoids permitting seepage of transudate into the peritoneal cavity [26, 27]. The extent of ascites' development is dependent on the level of hydrostatic pressure [28] and less on oncotic plasma albumin pressure [26, 29]. Signs and symptoms of portal hypertension include haematuria, dysentery, bloody vomitus due to spontaneous rupture and bleeding from varices, encephalopathy due to abnormal liver part and thrombocytopaenia. Factors such as abnormal increase in nitric oxide production and circulation of endogenous vasoconstriction such as catecholamines, leukotrienes and angiotensin 2 enhance hepatic vascular resistance and portal hypertension [xxx, 31].
three.1.i Pathogenesis of hepatorenal syndrome in ascites
One of the complications of activation of RAAS and SNS in cirrhosis is the resultant renal vasoconstriction leading to subtract in renal perfusion and glomerular filtrate rate which progresses to renal damage [21, 22, 32, 33]. In hepatorenal syndrome, in that location are no significant morphological changes in renal histology, while the patients largely retain normal tubular function [5, 21]. The kidney analyte and serum creatinine concentration does not increase until the glomerular filtration rate becomes markedly reduced below 40 ml/min [22]. Most patients with cirrhosis have their creatinine level beneath 1.2 mg/dl, and diagnosis of HRS is only made when the creatinine concentration is higher than 1.5 mg/dl in the absence of other complicating aetiologies [22]. Hepatorenal syndrome manifests in two different types in cirrhotic patients. Type I HRS is a fulminating grade of the disease rapidly progressing to astute renal failure often precipitated past variceal bleeding, septic infection and spontaneous bacteria peritonitis with poor prognosis of days to weeks [22]. Type 2 is a more than chronic form of HRS. Well-nigh patients with this form of disease have a more stable creatinine concentration with only signs of refractory ascites due to unresponsive diuretics [34, 35].
With advancement in cirrhosis, in that location is also progressive increase in sodium and water reabsorption and subtract in renal claret flow and glomerular filtration [36]. Approximately 20% of cirrhotic patients with refractory ascites progress to HRS which results from severe liver and systemic circulatory dysfunction [28]. Hepatorenal syndrome results from marked overactivity of RAAS, SNS, AND and other endogenous vasoconstrictor factors which exceeds renal production of vasodilatory substances [PGE2, prostacyclin, nitric oxide]. The imbalance from renal vasodilatory mechanism and the intrinsic vasoconstrictor enhances vasoconstriction and hypoperfusion and decreases GFR with ultimate event of renal failure [22].
Advertisement
four. Diagnosis of ascites
Usually in that location is no laid down procedure on the steps to diagnose ascites; however a systematic approach applied in various disease conditions is advantageous in making appropriate diagnosis. A step-by-stride approach normally starts with concrete test.
4.ane Algorithm of diagnosis in ascites
four.1.1 Physical examinations
In physical examination, the patient is examined for the presence of ticks and fleas which would contribute in physical discomfort of the pet. Ticks' infestation contributes in depletion of blood book and anaemia. Anaemia is detected by the appearance of pale mucous membrane of the eye and the gum. Ectoparasitism from ticks' infestation may effect in malnutrition due to contest with the host for essential nutrients necessary for the synthesis of protein and albumin. This could result in hypoalbuminaemia/hypoproteinaemia and a decrease in plasma oncotic pressure level enhancing vascular permeability and seepage of fluid in the intestinal crenel. A distended or pulsating jugular vein in the cervix region may bespeak cardiovascular aberration. Yellowish discoloration of the eye indicates jaundice and hepatic disease. Generalised lymphadenopathy may propose lymphosarcoma and other inflammatory illness weather condition. A "standback" ascertainment reveals cases of dyspnea due to abdominal deportation of the diaphragm into the thoracic cavity compromising respiration. Respiratory distress could manifest in the form of rapid panting. Such status presents a divergence from the normal respiratory pattern, from coastal to costo-intestinal or intestinal blueprint. Blackness tarry-coloured faeces from gastrointestinal bleeding may signify ancylostomosis and portal hypertension. Concrete examination of the trunk reveals a distended abdomen. The content of the belly could either be by pregnancy, abdominal masses, fluid of diverse consistencies or organ enlargement. The diagnosis of ascites starts from differentiating these possibilities through various procedures. Beginning is to carry out abdominal ballottement using clinched fist. This technique tin can be used to differentiate intestinal masses from fluid. It tin exist used with other laboratory tests such as pregnancy exam to rule out pregnancy. It however has some limitations in differentiating abdominal masses from organ enlargement. Abdominal ultrasound is a better choice in differentiating abdominal contents. Information technology has been proven effective in the detection of ascetic fluid, its site of product and differentiation of austere nature from transudates and exudates [xi]. A recent research has shown the possibility of the employ of echotexture of ascetic fluid in the detection of the cause of ascites in patients [11]. Abdominal paracentesis however is a very useful technique in differentiation of austere fluid [28].
iv.1.2 Guidelines for paracentesis in a domestic dog (author'southward personal experience)
A well-applied paracentesis without contamination of intestinal content is essential in differentiation of ascetic fluid. To achieve this, the following steps should exist strictly practical:
-
First apply caution by the use of proper restrain technique on the dog.
-
Gently place the dog on a lateral decumbency exposing the larger part of the ventral belly.
-
Swab the ventral abdomen less covered with haircoat, along the linea alba down to the ventral abdomen between the left and right hindlimbs. (Linea alba is the preferred site of paracentesis due to its less vascularisation and less chance of contamination of the fluid with blood from puncture vessels and intestinal organs when approached through a different site on the abdomen.)
-
Puncture the linea alba using a 21 gauge needle and ten mL gauge syringe, and aspirate the fluid.
-
Decant the content of the syringe into a clean and well-labelled tube for laboratory investigation.
-
Request for cytology of the fluid (Figure 1).

Figure i.
Removal of ascites through the linea alba in an Alsatian brood of dog.
4.one.3 Diagnostic fluid markers in ascites
The colour of ascetic fluid is a very essential mark in the diagnosis of the cause of ascites. The color ranges from clear fluid to yellow, reddish and opaque with flakes of fibrin and debris depending on the aetiology. Information technology is therefore important to observe the above guidelines in paracentesis in order to avoid false discolouration of the fluid, thus affecting correct diagnosis. Various colours of ascetic fluid signify a different aetiology equally shown below [37]:
-
Pinkish discolouration of the fluid: This is oftentimes seen in cases of exudation of fluid from bacterial infection which may become purulent. The exudates are ofttimes turbid in consistency and contains more than 2.0 gm of protein and greater than 6000 cells/μL equanimous mostly of neutrophils with bear witness of +++ bacterial infection. This type of fluid is considered a medical emergency to prevent evolution of sepsis.
-
Clear straw-coloured fluid: This blazon of fluid is described as modified transudate often characterised by the presence of fibrin cells and white blood cells such every bit neutrophils and lymphocytes. It is often seen in cases of long-standing ascites from diverse conditions including correct-sided heart failure, malignant growth and hepatic affliction giving adventure to invasion of fibrinogens.
-
Clear opaque fluid: This fluid is described as collection of pure transudate into the peritoneal crenel free from contamination except with few invasions of mesothelial cells and tissue macrophages. This ascites may be seen in cases of portal hypertension, hepatic diseases, osmotic gradient deficit (hypoalbuminaemia), protein losing enteropathy, kidney impairment and albuminuria.
-
Reddish discolouration of fluid: This is seen in cases of haemorrhages and collection of frank blood in the peritoneal cavity due to conditions of trauma, coagulopathies and claret and blood vessel neoplasm. The fluid contains high levels of cells mainly cerise blood cells with PCV being above 20%.
-
Greenish discolouration of fluid: This is seen in cases of rupture and seepage of bile into the peritoneal cavity.
-
Milky/slightly xanthous discolouration: This describes a condition of collection of lymph in the peritoneal crenel due to trauma, infection, cancer or right-sided middle failure. This type of exudates is turbid and opaque and is oft described as chyle. It gives a positive outcome in Sudan III stain examination for lipids due to the loftier level of lipid in the fluid.
4.ane.4 Clinical exam (writer's personal experience)
Clinical examination is considered a useful tool in the identification of the cause of ascites. An elevated temperature would signify an underlying infectious or inflammatory condition such as bacterial tuberculosis. An elevated capillary refill fourth dimension would signify a decreased circulatory volume equally a event of cancerous or infectious status. Auscultation of the oestrus reveals various cardiovascular diseases such as muffled heart sound which is consistent with pericardial effusion and cardiac tamponade. Heart murmurs or irregular heartbeats are suggestive of right-sided center failure. An elevated heartbeat or tachypnoea may outcome from dyspnea due to cranial displacement of the diaphragm into the thoracic crenel. Cardiovascular abnormalities are confirmed through the utilize of electrocardiograph and echocardiography.
4.1.5 Biochemical investigation in ascites (writer'southward personal experience)
The conclusion of biochemical profile such as the liver enzymes, full protein level, SAAG, albumin concentration, full bilirubin and kidney analytes such as creatinine and urea levels is useful in the diagnosis of the cause of ascites.
4.1.6 Serum ascites albumin slope (SAAG)
Serum ascites albumin gradient is presently the best tool in diagnosis of the cause of ascites especially that from portal hypertension [38]. A SAAG value of <1.1 g/dl or eleven yard/l indicates causes of non-portal origin such as malignancy, etc. [5]. Gradients >1.1 g/dl or xi g/l signal ascites of portal hypertension.
4.1.7 Total protein
Although the traditional classification of ascites according to the transudate and exudate concept has almost phased out following the introduction of SAAG, it however still has relevance in clinical practice for comparison and prognostic value. Concentrations beneath 15 one thousand/fifty are often associated with hazard of spontaneous bacteria peritonitis in cirrhosis [5, 39].
4.one.8 Triglycerides
An elevated triglyceride concentration in ascetic fluid above 2.two mmol/l indicates chylous ascites [38]. Chylous ascites is mutual in neoplastic cases although information technology may occur in 6% of cirrhosis [40].
4.one.9 Urea and creatinine
Elevated levels in urea and creatinine concentrations in ascetic fluid indicate prerenal failure due to peritoneal absorption of urea [41]. Urinary ascites is often associated with bladder changes and urethra obstruction [41, 42].
4.1.10 Cytology
Cytology of austere fluid is often indicated in suspected malignancy and idiopathic cases. Positive cytology is highly indicated in suspected cases of peritoneal carcinomatosis. The sensitivity of cytology tin can be enhanced by examination of iii samples from separate paracenteses [38]. The sensitivity is as well enhanced by prompt analysis of ascetic fluid and obtaining big book of upwards to l–g ml in patients with initial negative result.
iv.ane.11 Diagnostic laparotomy
Diagnostic laparotomy is indicated in cases of difficulty in identification of the aetiology of ascites. Ofttimes laparotomy presents adequate visual inspection of the peritoneal cavity and avenue for biopsy collection for histological and microbiological studies [38]. Diagnostic laparotomy provides basis for effective diagnosis of peritoneal carcinomatosis, tuberculous peritonitis, etc. [43, 44].
iv.1.12 Leucocyte esterase reagent strip
Several studies have shown the usefulness in the use of leucocyte esterase reagent strip in diagnosing spontaneous bacteria peritonitis and in urinary analysis with sensitivity ranging from 80 to 93% and specificity 93–98% [45]. The negative predictive value is markedly high from 97 to 99%, a good measure for an ideal tool to dominion out SBP [45]. Recent evolution has discovered an ascite-specific reagent strip with a cut-off value of 250 cells/mmthree which would farther enhance diagnostic accurateness [46].
4.ane.thirteen Platelet indices
Increased platelet indices such as hateful platelet volume and platelet distribution width have been observed to increase in cirrhosis. The usefulness of the platelet indices is yet to be fully elucidated but has shown propensity as a potential diagnostic tool [47].
4.one.14 Tumour markers
The use of neoplasm markers such equally alpha - feto protein, des-gamma-carboxy prothrombin, cancer antigen 125, etc. in the diagnosis of cancer in ascetic fluid is presently a subject of controversy among several researchers. Although the increased level of these markers is associated with underlying malignancies, elevated levels are likewise observed in other conditions such as pancreatitis, gastritis, etc. [48].
four.1.fifteen Imaging tools
Radiographical imaging is useful in detailing small amounts of ascetic fluid as well as diagnosis of aetiology of ascites [49]. Intestinal ultrasonography can detect as little as 100 ml of intraperitoneal fluid [50]. The sensitivity of radiography is enhanced through the use of computed tomography which detects minute quantities of ascetic fluid. Radiography enhances the picture of internal organs and aids in detection of cirrhosis, intra-abdominal tumour and organ enlargements. Thickening of mesentery and bowel wall, matting of bowel loops and enlargement of mesenteric lymph nodes may provide a guide in the diagnosis of tuberculosis peritonitis in afflicted patients. A dissimilarity computed tomography (CT) may be used to demonstrate enhancement of peritoneal lining. Cases of cirrhosis and large hydrothorax can be diagnosed with the assist of scintigraphy with technetium sulphur colloid or radiolabelled albumin [half-dozen].
4.i.sixteen Bacterial culture
Spontaneous bacterial peritonitis may arise due to decreased level of compliments which serve equally antibacterial factors in ascetic fluid. Suspected cases of SBP are cultured in both aerobic and anaerobic blood media for isolation of organisms [51]. Cultured ascetic fluid should be subjected to sensitivity test to identify effective antimicrobiological agent in treatment.
The Dna of
Advertisement
v. General treatment options in ascites
Ascites is treated symptomatically while addressing the primary cause of the condition. Efforts are geared towards relieving manifesting symptoms and preventing progression of ascites. The main goal in congestive heart failure is to improve cardiac contractility, normalise cardiac arrhythmias and enhance cardiac output. Cardiac drugs such as dopamine and digoxin can be used at recommended dosages in cases of congestive center failure in dogs. Dogs with right-sided heart failure should be placed on cage rest and on sodium-restricted diet [52]. Paracentesis is practical to relieve abdominal tension on the diaphragm and enhance normal respiration. Repeated paracentesis is non required except in cases of failing treatment [52]. Paracentesis should not exceed 1.0 kg weight per 24-hour interval for dogs with both ascites and peripheral oedema and less than 0.5 kg weight per day for patients with but ascites. Serum albumin sometimes is depleted during paracentesis and therefore should exist monitored and replaced intravenously in case of depletion at the same quantity of fluid removed. The administration of albumin dosed at 1.five yard/kg on the first day and 1.0 g/kg on the 3rd day ensured renal preservation and reduced mortality [53]. In cases of syncope, a balanced isotonic crystalloid fluid replacement such as Plasma-Lyte A, Normosol R and 0.ix% saline may be used in resuscitation and other conditions such every bit hypernatraemia, hyponatraemia, hypercalcemia, metabolic alkalosis or oliguria renal failure. Diuretics are used in addition to paracentesis to relieve ascites. Diuretics may be dosed once daily. Spironolactone has a one-half life of 24 hours and is given at the dose of 100 mg/solar day max 400 mg/mean solar day for response [54]. The dose may exist spread out every 2 hours stat in dogs nether hospitalisation and close monitoring at 2 mg/kg × im and at iii mg/kg × per os at night. Spironolactone could be substituted with either triamterene or amiloride since both drugs have expert antagonistic issue on aldosterone action on the collecting tubules [55]. Furosemide is frequently the first line of handling in cases of ascites with a one-half life of i.5 hours and given at the dose of 40 mg/mean solar day and max 160 mg/ day in case of nonresponders to furosemide [39]. The dose may also be spread in divided doses of 3 mg/kg × IV every 2 hours and at 4 mg/kg per bone at night. Bumetanide and spironolactone could be used in combination with furosemide at the ratio of 100:xl to reduce chances of furosemide resistance. The dose ratio ensures efficient natriuresis and period of water and also reduces the take a chance of potassium deficit from the use of furosemide [39, 56]. Other diuretics such as torsemide and bumetanide have shown meliorate efficacy than most diuretics [57]. Torsemide has a longer half life than both furosemide and bumetanide [57]. Patient with cirrhotic ascites often presents with complications of SBP, portal hypertension and HRS [28]. Cases without such complications are described as "elementary ascites" [58]. The standard treatment for SBP in humans involves immediate administration of third-generation cephalosporin such as intravenous ceftriaxone ane to two one thousand daily for v days [52]. The dose could exist given at 1 one thousand daily in dogs. The use of oral fluoroquinolones is as effective in the treatment of SBP [59, threescore]; alternatively piperacillin and tazobactam could be considered [61]. The choice of antibacterial agent depends on civilisation and sensitivity test to reduce problems of drug resistance. Antibody handling is usually given for an extended period to ensure consummate cure of the bacterial infection.
Portal hypertension is managed by the use of antihypertensive medications. A drug such equally metolazone (Mykron, Zaroxolyn) aids in the elimination of oedema in congestive middle failure. It enhances sodium excretion by inhibition of sodium reabsorption from the distil tubules, a function which is beneficial in renal conditions [55]. Mannitol (Osmitrol) inhibits tubular reabsorption of electrolyte by increasing the osmotic pressure of glomerular filtrate and urine output [55]. Cases of recurrent ascites in humans from portal hypertension may crave the use of TIPS [28]. TIPS functions as a side-to-side portacaval anastomosis between the high portal pressure terminate and low hepatic vein force per unit area cease, thereby effectively decongesting the portal system which may be useful in pets. A reduction in the portal hypertension brings a secondary decrease in RAAS activation and consequent increase in sodium excretion [62]. Persistent ascites from cirrhosis may be managed through liver transplant and removal of the damaged liver. The hepatic cells naturally possess high regenerative capacity and can regenerate after undergoing severe degenerative condition. The hepatocytes in addition can perform at total capacity even with few viable cells, and therefore liver transplant is only required as a last resort later on awarding of all remedial medications.
Renal failure is managed past controlling blood pressure level with drugs; avoid the employ of hepatotoxic medications in handling of ascites and the use of non-steroidal anti-inflammatory agents (NSAIDs) such as acetaminophen. Kidney dialysis is recommended in severe kidney damage. A continuous venovenous haemodialysis (CVVHD) is recommended compared to intermittent renal dialysis.
Cases of complications of encephalopathies from hepatic failure are best managed in intensive care units (ICU) [18]. Cases of early complexity of encephalopathy may be treated as outpatient; nevertheless such a patient is closely monitored for further deterioration to grade II encephalopathy which would crave prompt transfer to an intensive care unit of measurement. Such a patient is placed on routine bank check on mental balance, and signs of restlessness could be slightly sedated with low dose of brusk-acting benzodiazepines. Patients nether sedation are placed on undisturbed bed rest avoiding extensive motion which may enhance chances of intracranial pressure/hypertension. Dyspnea is prevented in late encephalopathy through placement of intratracheal intubation to avoid farther complications of aspiration pneumonia. The conditions of cerebral oedema and intracranial hypertension manifest at the late phase of encephalopathy and are prevented through routine checks on the patient's renal parameters; biochemical profile including liver enzymes, full protein, glucose, electrolytes and acid/residue; and neurological evaluations for signs of elevated levels [4]. Cases of severe haemorrhage issue from problems of coagulopathies which can be treated past addressing the coagulopathy through transfusion of coagulation products such as fresh frozen plasma and platelets and assistants of vitamin K. Severe conditions may exist boosted by transfusion of packed cerise blood cells. Continuous haemorrhage after massive replacement infusions may indicate possible retroperitoneal bleeding [18]. A adept number of herbal and antioxidant medications have shown to be beneficial in the treatment of ascites of hepatic origin. The use of these drugs remains controversial, merely despite this the drug N-acetylcysteine and
Conclusion: Ascites is a affliction condition commonly seen in pets of various age brackets with loftier incidences occurring in middle-aged dogs. Ascites is a common manifestation of a decompensate cirrhosis, cardiac diseases and several other aetiologies and is best diagnosed through established standard procedures of physical and clinical examinations, complete blood movie, cytology and various biochemical analyses. Contempo novel techniques such every bit platelet indices, leucocyte esterase reagent strip, tumour markers, bacterial DNA, cytokines and other proteins are available for the advancement of biochemical laboratory techniques and efficient diagnosis of ascites. Treatment is centred on effective diagnosis of the aetiology.
Advert
Acknowledgments
I sincerely admit the God Almighty for His enablement bestowed upon me during the course of this write-up.
Advertisement
Appendix
difficulty in breathing
degenerative condition in the brain
obstruction of the bile duct
red claret cell destruction
study of both the breadbasket and intestines
report of the blood
study of the nervous tissues
accumulation of fluid in the abdominal cavity
accumulation of fluid in the abdominal crenel
irregular heartbeat
closure or blockage peculiarly to terminate haemorrhage
problem with blood clotting mechanism
reversibly combined with a compound
compound in its natural form
not transparent, cloudy, filmy
the cause of a disease condition
area supplied with blood vessels
fluid produced from increased pressure level in the hepatic, portal vein (>8 mmHg) usually around twenty mmHg, low in protein (<xxx m/50), low in LDH, high pH, normal glucose and fewer cells
fluid actively secreted from inflammation or malignancy, rich in protein, lactate dehydrogenase, low pH (<vii.30), low glucose level and big numbers of white blood cells
pertains to the kidney
condition that affects both the liver and kidney
active compound in milk thistle herbal preparation
a poisonous species of mushroom
unknown origin
References
- 1.
Saravanan One thousand, Sarma Chiliad, Kumar M, Mahendran K, Mondal DB. Therapeutic management of ascites in dogs. The Indian Veterinary Journal. 2013; 90 (2):110-111 - 2.
Michael PW, Zenoble RD. Canine ascites. Digital Repository Iowa State University. 1982; 44 (1):3 - iii.
Pradhan MS, Dakshinkar NP, Naghaye UG, Bodkhe AM. Successful handling of ascites of hepatic origin in canis familiaris. Veterinary World. 2008; ane (1):23 - four.
Chalasani NP, Hayashi PH, Bonkovsky HL, Navarro VJ, Lee WM, Fontana RJ, et al. ACG clinical guideline: The diagnosis and management of idiosyncratic drug-induced liver injury. American Journal of Gastroenterology. 2014; 109 (7):950-966 - 5.
European Association for the study of the liver. EASL clinical exercise guideline on the management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome in cirrhosis. Periodical of Hepatology. 2010; 53 :397-417 - 6.
Sood R. Ascites: Diagnosis and management. Journal, Indian Academy of Clinical Medicine. 2000; 5 (1):81-89 - 7.
Christopher MM, Van Thiel DH. Cirrhotic ascites review: Pathophysiology, diagnosis and management. World Journal of Hepatology. 2013; v (5):251-263 - eight.
Ginés P, Quintero East, Approach V, Terés J, Bruguera M, Rimola A, et al. Compensated cirrhosis: Natural history and prognostic factors. Hepatology. 1987; 7 (1):122-128 - 9.
Planas R, Montoliu Due south, Ballesté B, Rivera M, Miquel Thousand, Masnou H, et al. Natural history of patients hospitalized for management of cirrhotic ascites. Clinical Gastroenterology and Hepatology. 2006; 4 :1385-1394 - 10.
Guevara M, Cárdenas A, Uriz J, Ginès P. Prognosis in patients with cirrhosis and ascites. In: Ginès P, Arroyo 5, Rodés J, Schrier R, editors. Ascites and Renal Dysfunction in Liver Disease: Pathogenesis, Diagnosis, and Treatment. 2nd ed. Malden, MA: Blackwell Publishing; 2005. Affiliate 21 - 11.
Mohammed SA, Caroline EA, Boushra HA, Elsafi AA. Radiology, diagnostic imaging and instrumentation. Global Periodical of Medical Research. 2013; 3 :3. version one.0 - 12.
Shanker Due south, Divya J, Pramod Kumar A, Bijoykumar B. Clinicopathological correlation of serum ascites albumin slope with ascetic fluid total protein in patients of ascites with portal hypertension attending a tertiary care infirmary in eastern Bihar India. International Journal of Advances in Medicine. 2017; 4 (3):842-846 - 13.
McNally PR. Gastrointestinal/Liver Secrets. 4th ed. Philadelphia, PA: Mosby Elsevier; 2010 - 14.
Shailja CS, David AS. "Cardiac Hepatopathy": A review of liver dysfunction in heart failure. Liver Research Open Journal. 2015; 1 (1):1-10 - 15.
Moitinho E, Escorsell A, Bandi JC, Salmerón JM, García-Pagán JC, Rodés J, et al. Prognostic value of early on measurements of portal pressure in acute variceal bleeding. Gastroenterology. 1999; 117 :626-631 - sixteen.
Runyon BA. Ascites and spontaneous bacterial peritonitis. In: Feldman Thou, Friedman LS, Brandt LJ, editors. Sleisenger and Fordtran's Gastrointestinal and Liver Illness. 9th ed. Philadelphia, PA: Saunders; 2010 - 17.
Fernandez-Esparrach 1000, Sanchez-Fueyo A, Gines P, Uriz J, Quinto Fifty, Ventura P, et al. A prognostic model for predicting survival in cirrhosis with ascites. Journal of Hepatology. 2001; 34 :46-52 - 18.
Gagen KS. Acute Liver Failure, Handling and Management. 2017. Available from: https://emedicine.medscape.com/commodity/177354-treatment#d1 - 19.
Bataller R, Arroyo V, Gines P. Management of ascites in cirrhosis. Journal of Gastroenterology and Hepatology. 1997; 12 :723-733 - 20.
Gentilini P, Vizzutti F, Gentilini A, Zipoli Chiliad, Foschi M, Romanelli R. Update on ascites and hepatorenal syndrome. Digestive and Liver Disease. 2002; 34 :592-605 - 21.
Ginès P, Schrier RW. Renal failure in cirrhosis. The New England Journal of Medicine. 2009; 361 :1279-1290 - 22.
Vicente AMD. Pathophysiology, diagnosis and treatment. Register of Hepatology. 2002; 1 (2):72-79 - 23.
Dudley F. Pathophysiology of ascites formation. Gastroenterology Clinics of North America. 1992; 21 :215-235 - 24.
Gines P, Fernandez-Esparrach Thou, Arroyo V, Rodes J. Pathogenesis of ascites in cirrhosis. Seminars in Liver Disease. 1997; 17 :175-189 - 25.
Casado M, Bosch J, Garcia-Pagan J, Bru C, Banares R, Bandi J, et al. Clinical events after transjugular intrahepatic portosystemic shunt: Correlation with hemodynamic findings. Gastroenterology. 1998; 114 :1296-1303 - 26.
Henriksen J, Siemssen O, Krintel J, Malchow-Møller A, Bendtsen F, Ring-Larsen H. Dynamics of albumin in plasma and ascitic fluid in patients with cirrhosis. Journal of Hepatology. 2001; 34 :53-60 - 27.
Kravetz D, Bildozola Thou, Argonz J, Romero Chiliad, Korula J, Munoz A, et al. Patients with ascites have higher variceal pressure level and wall tension than patients without ascites. The American Journal of Gastroenterology. 2000; 95 :1770-1775 - 28.
Pedersen JS, Flemming B, Møller S. Management of cirrhotic ascites. Therapeutic Advances in Chronic Disease. 2015; 6 (three):124-137 - 29.
Moore KP, Aithal GP. Guidelines on the direction of ascites in cirrhosis. Gut. 2006; 55 (Supplement half-dozen):vi1-v12 - 30.
Iwakiri Y, Groszmann R. The hyperdynamic circulation of chronic liver diseases: From the patient to the molecule. Hepatology. 2006; 43 :S121-S131 - 31.
Møller S, Henriksen J. The Systemic Circulation in Cirrhosis. Malden, Ma: Blackwell Publishing; 2005 - 32.
Henriksen J, Møller S. Alterations of Hepatic and Splanchnic Microvascular Exchange in Cirrhosis: Local Factors in the Formation of Ascites. Malden, MA: Blackwell Publishing; 2005 - 33.
Stadlbauer Five, Wright G, Banaji Grand, Mukhopadhya A, Mookerjee R, Moore K, et al. Relationship between activation of the sympathetic nervous system and renal blood flow autoregulation in cirrhosis. Gastroenterology. 2008; 134 :111-119 - 34.
Krag A, Bendtsen F, Henriksen J, Moller Southward. Low cardiac output predicts development of hepatorenal syndrome and survival in patients with cirrhosis and ascites. Gut. 2010; 59 :105-110 - 35.
Ruiz-Del-Arbol L, Monescillo A, Arocena C, Valer P, Gines P, Moreira V, et al. Circulatory function and hepatorenal syndrome in cirrhosis. Hepatology. 2005; 42 :439-447 - 36.
Wensing G, Lotterer E, Link I, Hahn E, Fleig W. Urinary sodium balance in patients with cirrhosis: Relationship to quantitative parameters of liver function. Hepatology. 1997; 26 :1149-1155 - 37.
Ettinger SJ, Feldman EC. Textbook of Veterinary Internal Medicine Diseases of the Dog and Cat. 6th ed. Vol. one. United states of america: Elsevier Saunders; 2005 - 38.
Oey RC, van Buuren Hour, de Human RA. The diagnostic work-up in patients with ascites: Current guidelines and future prospects. The Netherlands Journal of Medicine. 2016; 74 (viii):330-338 - 39.
Runyon BA. Management of adult patients with ascites due to cirrhosis: An update. Hepatology. 2009; 49 :2087-2107 - 40.
Laterre PF, Dugernier T, Reynaert MS. Chylous ascites: Diagnosis, causes and treatment. Acta Gastroenterologica Belgica. 2000; 63 :260-263 - 41.
Peeters P, Colle 2, Serinesael J, Verbeelen D. Relapsing ascites and uremia due to urinary bladder leakage. European Journal of Internal Medicine. 2001; 12 :60-63 - 42.
Snauwaert C, Geerts A, Colle I, Van vlierberghe H. Ascites not ever the usual suspect. Acta Gastro-Enterologica Belgica. 2012; 75 :45-48 - 43.
Han CM, Lee CL, Huang KG, et al. Diagnostic laparoscopy in ascites of unknown origin. Chang gung memorial infirmary 20 years feel. Chang Gung Medical Journal. 2008; 31 :378-383 - 44.
Yoon YJ, Ahn SH, Park JY, et al. What is the office of diagnostic laparoscopy in a gastroenterology unit? Journal of Gastroenterology. 2007; 42 :881-886 - 45.
Rerknimitr R, Limmathurotsakul D, Bhokaisawan Northward, Kongkam P, Treeprasertsuk S, Kullavainijaya P. A comparison of diagnostic efficacies among dissimilar reagent strips and automated prison cell count in spontaneous bacterial peritonitis. Journal of Gastroenterology and Hepatology. 2010; 25 :946-950 - 46.
Mendler MH, Agarwal A, Trimzi M, et al. A new highly sensitive signal of care screen for spontaneous bacterial peritonitis using the leukocyte esterase method. Journal of Hepatology. 2010; 53 :477-483 - 47.
Abdel-Razik A, Eldars Westward, Rizk E. Platelet indices and inflammatory markers in diagnostic predicators for austere fluid infection. European Periodical of Gastroenterology & Hepatology. 2014; 26 :1342-1347 - 48.
Huang LL, Xia HH, Zhu SL. Ascitic fluid analysis in the differential diagnosis of ascites: Focus on cirrhotic ascites. Periodical of Clinical and Translational Hepatology. 2014; ii :58-64 - 49.
Theoni RF. The function of imaging in patients with ascites. American Journal of Roentgenology. 1995; 165 :16-eighteen - 50.
Goldberg BB, Goodman GA, Clearfield Hour. Evaluation of ascites past ultrasound. Radiology. 1970; 96 :15-22 - 51.
Siersema PD, de Marie S, van Zeijl JH, Bac DJ, Wilson JH. Blood culture bottles are superior to lysis-centrifugation tubes for bacteriological diagnosis of spontaneous bacterial peritonitis. Journal of Clinical Microbiology. 1992; 30 :667-669 - 52.
Moore CM, Van Thiel DH. Cirrhotic ascites review: Pathophysiology, diagnosis and direction. World Journal of Hepatology. 2013; 27 (five):251-263 - 53.
Sort P, Navasa M, Arroyo V, Aldeguer X, Planas R, Ruiz-del-Arbol L, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. The New England Journal of Medicine. 1999; 341 :403-409 - 54.
Tsochatzis EA, Gerbes AL. Diagnosis and treatment of ascites. Periodical of Hepatology. 2017; 67 (one):184-185. DOI: 10.1016/j.jhep.2017.01.011 - 55.
Rahil Southward, Janice MF. Ascite. Drugs and affliction. Gastroenterology. Medscape. 2017. https://emedicine.medscape.com/article/170907-overview - 56.
Santos J, Planas R, Pardo A, Durández R, Cabré E, Morillas RM, et al. Spironolactone alone or in combination with furosemide in the treatment of moderate ascites in nonazotemic cirrhosis. A randomized comparative written report of efficacy and prophylactic. Journal of Hepatology. 2003; 39 :187-192 - 57.
Wargo KA, Banta WM. A comprehensive review of the loop diuretics: Should furosemide be offset line? Annals of Pharmacotherapy. 2009; 43 (eleven):1836-1847, 2009 - 58.
Salerno F, Angeli P, Bernardi G, Laffi Yard, Riggio O, Salvagnini M. Clinical practice guidelines for the management of cirrhotic patients with ascites. Committee on ascites of the Italian Association for the Study of the liver. Italian Journal of Gastroenterology and Hepatology. 1999; 31 :326-334 - 59.
Felisart J, Rimola A, Arroyo 5, Perez-Ayuso RM, Quintero Eastward, Gines P, et al. Cefotaxime is more effective than is ampicillin-tobramycin in cirrhotics with astringent infections. Hepatology. 1985; 5 :457-462 - 60.
Navasa M, Follo A, Llovet JM, Clemente 1000, Vargas V, Rimola A, et al. Randomized, comparative study of oral ofloxacin versus intravenous cefotaxime in spontaneous bacterial peritonitis. Gastroenterology. 1996; 111 :1011-1017 - 61.
Novovic S, Semb Southward, Olsen H, Moser C, Knudsen J, Homann C. Beginning-line treatment with cephalosporins in spontaneous bacterial peritonitis provides poor antibiotic coverage. Scandinavian Journal of Gastroenterology. 2012; 47 :212-216 - 62.
Rossle K, Siegerstetter V, Huber Thousand, Ochs A. The first decade of the transjugular intrahepatic portosystemic shunt (TIPS): Land of the art. Liver. 1998; xviii :73-89 - 63.
Chronic Liver Illness. https://en.wikipedia.org/wiki/chronic_liver_disease
Submitted: July 26th, 2018 Reviewed: January 28th, 2019 Published: May 14th, 2019
© 2019 The Writer(s). Licensee IntechOpen. This chapter is distributed under the terms of the Creative Eatables Attribution 3.0 License, which permits unrestricted use, distribution, and reproduction in whatsoever medium, provided the original work is properly cited.
Source: https://www.intechopen.com/chapters/66978
Posted by: grangerapoing.blogspot.com
0 Response to "What Is The Pagan Significance Of Tearing Out An Animal's Chest Cavity"
Post a Comment